Most people in today’s world who have an eating disorder have heard that voice. A lot of people who don’t have an eating disorder have likely heard it too.
Not feeling thin enough is an obvious driver of eating disorders such as anorexia, bulimia and binge eating disorder. We live in a culture where we’re surrounded by a surplus of food with the most readily available foods such as take aways and things in wrappers being processed and full of fat and sugar. Yet, we’re pressured to be thin. Thin bodies are associated with self-discipline, with eating ‘good’ foods like lean meat and salads, with being active. Fat bodies are associated with a lack of control, with eating ‘bad’ foods like chips and chocolate, with laziness and avoidance of exercise. This drives people to unhealthy dieting, which can lead to an eating disorder.
Yet, thin societal ideals have only been around for a couple of centuries. Eating disorders haven’t always mainly been about thinness. They might instead be related to other feelings of not being enough. Examples throughout history of anorexia mirabilis, ‘wondrous’, ‘miraculous’ or ‘holy anorexia’ were more to do with not feeling holy or special enough.
The earliest known example is Blaesilla, a Roman woman who lived in the 4th century. She was the daughter of Paula of Rome, a saint and Desert Mother, who became abbess of a convent of nuns under the strict ascetic regime of Saint Jerome.
Paula of Rome and her nuns
Blaesilla led a ‘merry life’ until, aged eighteen, she married, was widowed, then criticised by Jerome for her ‘frivolous’ behaviour. Like her mother, she began to follow the ascetic methods of Jerome. She took to wearing plain clothes, studied hard, prayed harder and fasted to extremes. The extremity of her fasting killed her at the age of twenty. It might be argued that not feeling holy enough in the face of the demands of Jerome and the status of her mother drove her to prove her worth by self-starvation.
It might, perhaps, be said that feelings of not being holy enough also drove other female religious figures in medieval times, such as Catherine of Siena, to starve themselves to death. Catherine gave up meat at a very young age. In her later life, she barely left her cell and went almost entirely without food or sleep. She wrapped an iron chain around her body and scourged herself until she bled. Still, her penances weren’t enough. She eventually came to reject all food except for the bread and wine of the Eucharist, for which she, unsurprisingly, developed such an extreme and unseemly hunger some members of the clergy refused to give it to her. She died at the age thirty-three.
In Hellenistic culture and during the medieval period, restrictive dieting and the resulting thinness were associated with self-discipline and religious purity. Fasting and being thin made a person feel more holy, more enough.
The ‘fasting women’ of the seventeenth and eighteenth centuries, such as Martha Taylor, Anne Moore and Mary Thomas, who were renowned for surviving for extended periods of time without food were seen as living ‘wonders’ or ‘miracles’. Their fasting has been linked to illness and trauma, but also might be seen to be related to feelings of not being enough.
At this point, it’s worth highlighting that the majority of historic examples of people suffering from eating disorders are female and this continues today with 75% being women and 25% men. I believe this to be a reflection of the patriarchal nature of Western European culture since the dominance of Christianity.
Women, subordinate to men, have rarely felt they are enough. Thus, female religious, unable to become clergy, turned instead to proving their worth and holiness through extreme ascetic practices including self-starvation. Later women starved themselves as they had no other means of leading wondrous lives.
Over the last couple of centuries, the media has constantly been sending out the message that we’re not enough – not thin enough, not fit enough. Social media influencers reinforce this by showing off their toned bodies and food and exercise regimes. This can lead to restrictive eating and over-exercising and thereby to Anorexia nervosa and Anorexia athletica. Feeling we are not enough can also cause us to comfort eat, over-eat, or binge, which can lead to Bulimia nervosa (for those who purge) or to binge eating disorder. It is common for a person to switch between eating disorder diagnoses.
***
My eating disorder began when I was six as a slightly tubby autistic child. I was neither thin enough nor normal enough to fit in, so I got bullied. This led to comfort eating, binge eating, then to binge eating disorder. I started restricting and over-exercising when I was thirteen because I wanted to be thinner and more normal (thin = normal) but the binger won out again. In my twenties I ‘conquered’ the binging at the price of slipping into mild anorexia.
My life continued to be dominated by destructive patterns of dietary restriction, excessive exercise and binge drinking. These were driven by a feeling of failure – not getting funding for my PhD, not succeeding in a career with horses, not being able to make a living as a writer, failing at a second attempt at a career – this time in conservation.
Taking up strength training and adopting a monastic lifestyle helped. Instead of being thin, I determined to become a strong vessel for the inspiration of my Gods. But I was never monastic enough. I was never holy enough.
Having moved on from monasticism I can see how much of my asceticism – giving up certain foods and alcohol, keeping a strict meditation and exercise regime, getting rid of clothes and books and cutting out entertainment – was driven by the same restrictive principle that, in extremes, becomes anorexia, starving oneself of all life’s sustenance.
The apogee was when I spent nine days in meditation at the Abyss with a spear in my belly – a representation of the impulse within that can lead to death through self-starvation.
Having realised that monasticism wasn’t entirely healthy for me and decided to focus on becoming a good shamanic practitioner, the voice remains, telling me I’m not shamanic enough. Trying to force upon me its ideals of what a shamanic practitioner should look like (which, of course, is thin, signifying purity and self-discipline). Mocking my more muscular body and red face. In opposition to this, my Gods and spirits tell me I have to be strong in body and mind for myself and my clients.
As I’ve deepened into my path, the unwavering support and unconditional love of my patron God, Vindos, my helping spirits, my mum, a good friend and my shamanic mentor, and kind words from clients, have helped me to feel more worthy, more enough.
I’d like to say that I have reached a point where I feel I’m of intrinsic worth and value but I’m not there yet. Being able to control my weight and my exercise routine remain a crutch. But being able to say “I’m enough” occasionally is a step forward.
A few months ago, I learnt how the new weight loss jabs not only help people to lose weight but dampen ‘food noise’. I hadn’t heard of ‘food noise’ before and quickly found out that the term was coined in the 2000s and relates to ‘food-related intrusive thoughts’ – the constant chatter about food that goes on in a person’s mind even when they’re not hungry. I recognised it immediately as something I used to experience (along with ‘alcohol noise’) and still experience to a certain degree. It has been labelled in eating disorder communities as ‘the eating disorder voice’.
Other the past few years, I had worked out that my food and alcohol related thoughts were just a couple of the varieties of the many types of noise generated by my over-thinking mind and had learnt to quieten them with meditation. Thus, I was shocked and intrigued to find out that an injection can mimic the effects of a practice I had taken a number of years to develop and still struggle with. This got me researching how the weight loss jabs work and how they affect the same neural pathways that are affected by meditation.
The medications in the weight loss injections are called GLP-1 receptor agonists. They are synthetic variants of GLP-1, an essential gut hormone, which lowers blood sugar, reduces appetite, and brings about feelings of satiety. Variants include semaglutide (Ozempic and Wegovy) and tirzepatide (Mounjaro).
When a person eats a meal, GLP-1 is released, and travels through the bloodstream and the vagus nerve to the brain, where it causes appetite suppression. It also goes to the pancreas, which produces insulin, lowering blood sugar.
GLP-1 ‘effectively shuts down areas in the brain involved in feeding response, homeostatic controls, energy balance and decision-making about food—as well as the liking and wanting of food and impulsive behaviours associated with eating.’ Thus, it dampens cravings and food-related thoughts.
Researchers have identified that GLP-1 shuts down the Default Mode Network – the background setting of the brain which drives mind-wandering, ruminating on the past, planning for the future, and self-reflection. This is responsible for us getting stuck in negative thought loops and food-related thoughts.
Like GLP-1, meditation, which involves training the mind to concentrate on one object of thought of a time, also shuts down the Default Mode Network. It not only stops ‘food noise’ but all other types of noise as well.
GLP-1 has also been shown to have an effect on the reward pathways that are not only associated with addiction to food but with other addictions. ‘Neurons that produce dopamine—a chemical with pivotal involvement in motivation and pleasure—project to the nucleus accumbens, a midbrain structure important for experiencing reward… Like other brain structures, the nucleus accumbens has GLP-1 receptors. Studies have shown that in animals, dopamine release peaks after they eat a sweet meal of sucrose—and after they are exposed to cocaine or opioids.’ GLP-1 dampens this effect, meaning the peak to such rewards is no longer received, weakening these pathways.
Meditation strengthens our ability to recognise cravings as just thoughts and not to act on them, thus weakening the neural pathways of food addiction. Both could thus be helpful for people with binge eating disorder and bulimia.
It’s notable, here, that restrictive eating disorders, such as anorexia, re-wire the brain to get the dopamine hit from restricting food intake and / or over-exercising to lose weight. Meditation can also help with addiction to restricting and excessive exercise.
It has been shown that people who use weight loss injections usually gain weight afterwards if they do not continue to follow a healthy lifestyle. Combining taking a GLP-1 receptor agonist with learning meditative techniques can help people to lose weight and keep the weight off.
In the previous post, I talked about my personal experiences of an eating disorder, which began as binge eating disorder, then developed into mild anorexia. In this article, I’m going to be exploring the context of its development in relation to the rise of eating disorders in the 20th century and their prevalence at this time. I will begin by outlining what eating disorders are and how the different types of eating disorders are currently defined. I will then provide a brief history of eating disorders, focusing on how the shift of cultural ideals from fuller forms towards thinness has led to their proliferation over the last century. I shall discuss how the flawed BMI model has led to the demonisation of obesity and to healthy people being shamed as overweight and obese and to developing eating disorders. I will then talk about the disturbing phenomenon of the deification of anorexia as the goddess Ana, within the pro-Ana movement. Finally, I will focus on how the decline of religion in Western Europe has led to size becoming a religion, with its own commandments on food and exercise, as voiced by new idols on social media.
What is an Eating Disorder?
An eating disorder is defined by the Oxford Language Dictionary as ‘any of a range of mental conditions in which there is a persistent disturbance of eating behaviour and impairment of physical or mental health.’
Eating disorders often develop as ways of managing difficult or overwhelming emotions that stem from stress and trauma. They can be precipitated by dieting and may or may not be related to cultural ideals of thinness.
An eating disorder differs from dieting and other forms of disordered eating such as skipping meals, in terms of the severity, frequency and duration of the symptoms, the levels of psychological and physical stress, and the impact on the person’s capacity to function and their relationships.
The Types of Eating Disorder
The main types of eating disorder are anorexia, bulimia, and binge eating disorder. In the UK, two resources are used to diagnose eating disorders: the Diagnostic and Statistical Manual of Eating Disorders, 5th Edition (DSM-5) and the International Classification of Diseases, 11th Edition (ICD-11).
Anorexia is defined by ‘the restriction of energy intake relative to requirements leading to a significantly low body weight’, ‘intense fear of gaining weight’ and disturbance in perception of body weight and shape. Other symptoms include: amenorrhea, digestive issues, dizziness, fainting, feeling cold and numb, poor circulation and dry skin. In severe cases, anorexia can lead to osteoporosis, organ failure, cardiac arrest and death. Around 5% of patients with anorexia die within four years of receiving a diagnosis.
The main diagnostic criteria of bulimia are ‘episodes of binge eating’ followed by ‘inappropriate compensatory behaviour’. Binge eating is defined as eating within a 2-hour period ‘an amount of food that is definitely larger than what most individuals would eat in a similar period of time under similar circumstances’ and by ‘a sense of lack of control of overeating during the episode’. Compensatory behaviours include: vomiting, misuse of laxatives, fasting and excessive exercise. These episodes are driven by concerns about body weight and shape. They must take place at least once a week for three months to warrant a diagnosis. Other symptoms are similar to anorexia and self-induced vomiting can also cause a sore throat, swollen glands, tooth erosion, Russel’s sign on the hands and electrolyte imbalances.
The diagnosis of binge eating disorder is also based upon ‘recurrent episodes of binge eating’. These are not followed by compensatory behaviours. Binge eating episodes must be associated with three or more of the following criteria: ‘eating much more rapidly then normal, eating until feeling uncomfortably full, eating large amounts of food when not feeling physically hungry, eating alone because of feeling embarrassed by how much one is eating, feeling disgusted with oneself or very guilty afterward’. Marked distress about the binge eating must be present and the episodes must take place at least once a week for at least once a month. Binge eating disorder can lead to excessive weight gain and thus to high blood pressure, high cholesterol levels, breathing issues, joint problems, digestive diseases such as gallstones and gallbladder disease and type two diabetes.
There are also a number of Other Specified Eating and Feeding Disorders (OSFED). These include atypical anorexia wherein ‘the criteria for anorexia are met, except that despite significant weight loss, the individual’s weight is within or above the normal range’, bulimia (of low frequency and/or limited duration), binge eating disorder (of low frequency and/or limited duration), purging disorder, night eating syndrome, pica, rumination disorder, Avoidant/Restrictive Food Intake Disorder (AFRID), orthorexia and Unspecified Feeding or Eating Disorder (UFED).
A History of Eating Disorders
It’s likely that humans have restricted food intake, binged, purged, and over-exercised as a form of relief from stress and trauma since we have existed. However, for the most part, people did not engage in such behaviours to be thin.
Venus figurines, with large bellies, breast and hips, suggest that larger body shapes were idealised during prehistoric times. This might relate to food scarcity and to larger forms being associated with fertility and survival.
Venus of WillendorfVenus of Hohle Fells
Religious fasting has long been a common practice and differs from an eating disorder as it involves a conscious choice to bring a person closer to the divine rather being a coping mechanism or a method of weight loss. However, it can develop into an eating disorder when it becomes an addiction and spirals out of control and manifests as self-starvation.
From the Hellenistic period, we have the first records of religious fasting being taken to the extremes of emaciation and starving. Blaesilla, a Roman woman who followed the ascetic practices of Saint Jerome, starved herself to death. This has been interpreted as an early example of anorexia.
We also find examples of binging and purging that bear similarities to bulimia in wealthy cities such as Ancient Rome. The Roman emperor, Vitellius, was renowned for having three or four feasts a day, made possible by his vomiting. The emperor, Claudius, never left a meal until overfed, after which ‘a feather was placed in his throat to stimulate his gag reflex.’ These behaviours have more to do with gluttony – emptying one’s belly in order to fill it with more food – than with bulimia as a mental illness outside their control.
In medieval times, extreme ascetic practices remained common. Around the 10th century, Saint Wilgefortis, ‘bearded virgin’, starved herself to avoid marriage, leading to hair growing all over her body (a phenomenon known as languo – the body’s response to fat loss in order keep warm), including her face, leading to her growing a beard. Saint Catherine of Siena famously starved herself to death in 1380, attempting to survive only on the eucharist. This phenomenon has been referred to as anorexia mirabilis ‘holy anorexia’.
Saint WilgefortisSaint Catherine of Siena
Intriguingly, in medieval tales wild men and woman who become geilt or wyllt ‘mad’ such as Suibhne Geilt, Mis, Myrddin Wyllt, and the knight, Owain, who retreat in madness into the wilderness, are described as hairy. This, no doubt, was caused by them living in a state of near-starvation. Living in the wild and extreme fasting are associated with initiation in some cultures. This might be seen as a temporary state of anorexia, which reaches an end when the person has a religious experience and returns to their community.
The illness we now know as anorexia nervosa was first described by Richard Morton, in 1689, in relation to a male and female who lost their appetite and wasted away without physical explanation from nervous consumption. The term anorexia nervosa (a nervous loss of appetite)was coined by William Gull in 1873 in relation to case studies of young women, aged 16 – 23, who suffered from fatigue, loss of body mass and weakness.
These diagnoses bore no relation to societal ideals of thinness. Up until the nineteenth century, the ideal female body shape was curvy and voluptuous, as shown by statues and paintings of women with fuller figures. It was during the Victorian period that slimmer ideals came into vogue, with hourglass figures, and women cinching in their waists with corsets.
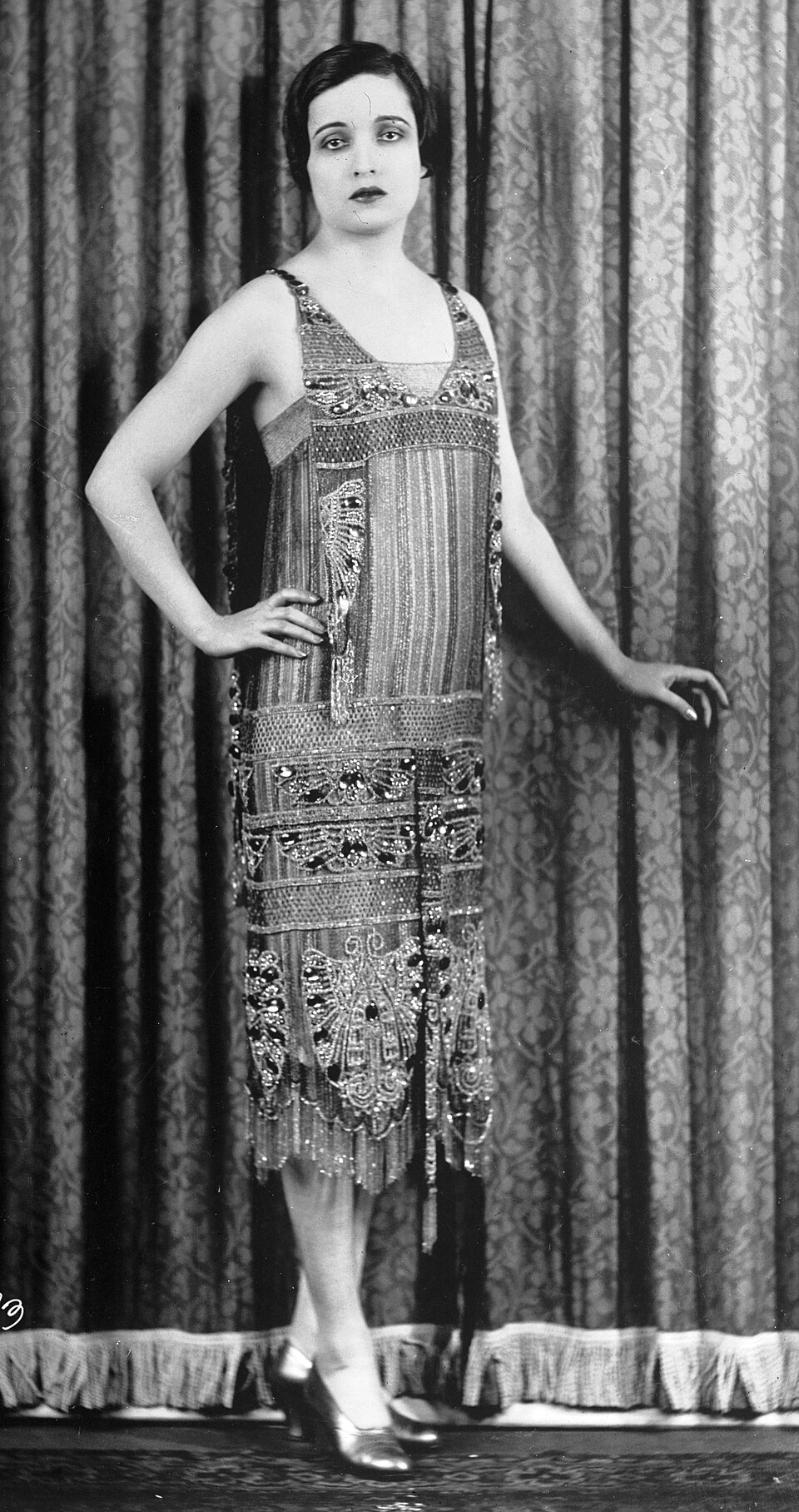
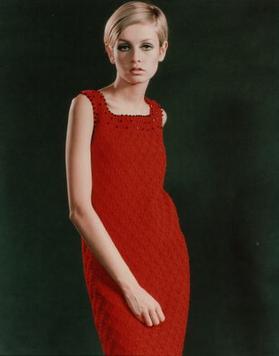
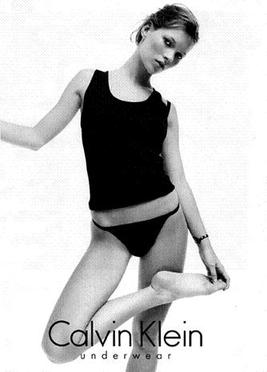
The thin ideal came into being in the 1920s with the flapper image focusing on a slender, boyish shape. In the 1960s, Twiggy provided the defining look. The apogee was the 1990s, when extreme levels of thinness were reached, with waif-like, clinically underweight models, referred to as heroin chic.
Flapper (Alice Joyce)TwiggyWaif – Kate Moss
The first case studies of binging and vomiting were recorded by Bliss and Branch in the 1960s, and by Ziolko during the 1970s. In 1979, Gerald Russell coined the term bulimia nervosa (bulimia means ‘ox-hunger’ and the term has been translated as ‘ravenous appetite’)in a paper covering 30 cases. Binge eating disorder was first described in 1959 by the psychiatrist, Albert Stunkard.
During the 1970s, an ‘epidemic of obesity’ was declared. People were labelled as overweight or obese and this led to many developing eating disorders.
A sudden rise in eating disorders, driven by the derogation of fat bodies and the glamorisation of near-anorexic bodies, was seen between the 1960s and 1990s. Their prevalence has risen even more sharply, by 15%, since 2000. This has been driven by the anxiety and social isolation of the COVID pandemic and by the influence of social media promoting unhealthy ‘thin’ and ‘fit’ ideals. A 2017 study by Hay, in the UK, found that that 8% of the cases were diagnosed with anorexia, 19% with bulimia, 5% with binge eating disorder, 5% with ARFID, and 47% with OSFED.
The Demonisation of Obesity
Unfortunately, fat-shaming has been around for a long time. In Spartan Greece, between the 6th and 2nd centuries BCE, slim, muscular physiques were favoured and fat people were shamed and even fined.
However, this was not the norm across cultures and history. Generally, fuller forms that were able to survive food shortages and harsh weather were lauded. In Western Europe, it was only during the nineteenth century, when the food supply became better, that a thin-waisted female figure was promoted and fatness became seen as a moral failing, associated with laziness and lack of self control. This was bound up with colonial values. Larger Black and Brown bodies were seen as dirty and undisciplined.
As the food supply has increased, so have the divisions between the cultural ideal of the thin white person and its antithesis – the fat (often Black) person. This has reached its height with the discourse around an ‘epidemic of obesity’.
Since the 1970s, obesity has been framed as a major health issue, stemming from unhealthy eating habits and a lack of exercise and associated with poverty. ‘Morbidly obese’ people, frequently depicted in the media as being lifted from their homes by ‘bariatric rescues’, are often seen as objects of ridicule and portrayed as being of demonic proportions.
In a 2025, in a report from the House of Commons Library on ‘Obesity Statistics’, 31% of women and 39% of men were labelled as overweight and 30% of women and 28% of men as obese. Adult obesity prevalence was shown to have risen from 15% in 1993 to 29% in 2022. This was shown to be associated with social deprivation, disability, ethnicity (‘people in Black ethnic groups have the highest rates of excess weight’) and a lack of education.
This discourse is based on the faulty BMI model hat originated as ‘the Quetelet index’ in 1932 when the Belgian sociologist, Adolphe Quetelet, designed the weight-to-height ratio (kg/m2) to define the ‘average man’ and measure population norms. Notably, it was created by a white man to find a norm amongst other white men. The term Body Mass Index (BMI) was coined in 1972 by Ancel Keys and used it as a tool for population studies on obesity.
Quetelet never intended his model to be used to used to measure individual health or body fat. It has increasingly been criticised because it does not take into account muscle mass, bone density or different body types.
Self-identified fat doctor, Astrıður Stefa´nsdottir, who, according to the BMI scale is overweight, yet is perfectly healthy, points out how the current ‘scientific’ position has led to fat people who are in in control of their fates in ‘the kingdom of the well’ being reduced to ‘patients’ in ‘the kingdom of the sick’ ‘under the management of medical personnel’.
During the 1960s, the Fat Liberation movement arose. This was deeply intertwined with the Black Rights movement. Both critiqued the hegemony of thin, white ideals and called for equal rights for fat and Black bodies. This has more recently developed into the Body Positivity movement and has led to the establishment of groups such as Health at Every Size (HAES) whose core principles are: weight inclusivity, health enhancement, respectful care, eating for well-being, and life-enhancing movement.
Sangerin Lizzo
The Deification of Anorexia
On the other extreme, the pro-anorexia or pro-ana movement began developing online in the early 2000s. Therein, anorexia is re-conceptualised as a lifestyle choice as opposed to an illness and is seen as a skill and as a religion.
These sites provide ‘thinspiration’ and actively encourage followers to under-eat and over-exercise, casting this in terms of self-discipline, and providing weight loss tips. ‘Anorexia is a skill, perfected by only a few. The chosen, the pure, the flawless.’ ‘Watch other people eat and feel superior. You don’t need that food!’ ‘The pain is necessary, especially the pain of hunger. It reassures you that you are strong, can withstand anything.’ They actively deny the danger to health and longevity of anorexia. ‘The bests anas never die.’
Anorexia is, even more disturbingly, portrayed as a religion with its own ruling goddess, Ana. She is viewed as a creator: ‘I (Ana) have created you, this thin, perfect, achieving child.’ She has her own version of the Ten Commandments, the Thin Commandments, such as ‘Thou shalt not eat without feeling guilty’. She is also viewed as a demoness who haunts and possesses.
This toxic online movement has led to people with anorexia seeing their illness as a lifestyle choice that lifts them above the herd, elevating them into a community who view themselves to be superior to the rest of food-eating society. This makes them less likely to seek treatment and can lead to death.
Size and Shape as Religion
Having studied the context, I now understand better the cultural milieu in which my eating disorder developed. I grew up in a Christian country with nominally Christian parents but, hating church parade with Brownies, reached the conclusion that the Christian God was not my God and didn’t entertain the thought that there might be others until I entered my mid-twenties.
My primary school was not religious. Instead, it was ruled by size and shape. A tubby child with a pot belly, I was bullied ruthlessly, called a ‘pig’. Comfort eating, due to bullying, led to binge eating, and I became overweight.
I’m not sure how long fat people have been identified with pigs. Wild boar and pigs are, contrarily, revered and cast as destructive in the Celtic tradition. Although swine were likely always seen as boisterous and as having voracious appetites, I imagine that it was not until they were penned that they were associated with dirtiness and laziness. How long insults such as ‘fat cow, ‘sow’ or ‘pig’, ‘eat like a pig’ and ‘pig out’ have existed, I remain uncertain.
During primary school and throughout high school, during the 1980s and 1990s, the female ideal did not seem to be based so much on skinny catwalk models as the Playboy or Barbie Girl aesthetic symbolised by Pamela Anderson. It was thin, blonde, tanned, with big boobs. Many of the girls at school bleached their hair, wore orange foundation and fake tan, lots of mascara and push-up bras. I didn’t adhere to this ideal. My first attempts to lose weight, at the age of thirteen, were driven more by the desire to evade bullying and to look like the thinner riding instructors at my riding school.
It was only when I started college that I started looking for ‘thinspiration’ to cultural idols. Again, these were not the thin female models from the catwalk. They were male figures from the eighties, rock and goth scene, such as David Bowie, Marilyn Manson and Richey Edwards, who sported an androgynous look. Looking back, this strikes me as odder than I remember, and leads me to the conclusion that I’m slightly gender fluid.
David Bowie – Ziggy StardustMarilyn Manson – Mechanical AnimalsRichey Edwards
At this time, I lost about three stone in six months, then continued to eat a restrictive diet, but yo-yoed up and down for a number of years due to binge eating and binge drinking, until I managed to get the binge eating under control. As my eating disorder shifted entirely into mild anorexia, I became underweight.
Androgyny suited my body because I’m naturally a rectangle shape with small breasts, not much of a waist, narrow hips and longish legs. I found that, when I gained weight mainly due to binge drinking, fat gathered around my stomach and on my face, making me look like a round-faced barrel on legs. When I lost weight again, I emulated a thin runner’s ideal. At present, at my ideal weight, eating healthily and strength training, my figure is more athletic and remains boyish.
Goth period prior to being underweightHigher end of normal weightIdeal weight
As a gym-goer I could say a lot about the religion of shape and size in gyms. In the 2010s, following the 2012 Olympics, the ‘strong not skinny’ movement formed a shift away from thinness towards strength and athleticism. This values function over form, body diversity, and mental strength. It celebrates a number of body shapes such as ‘toned’, ‘fit’ and ‘built’. Yet, ‘thick toned hour-glass figures’ for women, with narrow waists and well-developed glutes and thighs, have become the new ideal. This is something I certainly can’t achieve.
The ‘strong not skinny’ movement has been subject to critique due to its exclusion of thin people and replacing one unrealistic standard, thinness, with another, fitness, when the latter is difficult to attain for people with busy lives. It has also been seen as promoting restrictive dieting and excessive exercise.
Personally, I’ve found it’s helped me shift from being thin to being stronger and healthier. When I go to the gym, I don’t feel pressured to fit into any ideal. What I love about my gym is that there are bodies of all shapes, sizes and colours there, together, working out, without criticism or judgement.
A Better Religion
In Goodbye Ed, Hello Me, (ED stands for eating disorder), Jenni Schaefer writes about how she did not manage to recover from her eating disorder fully until she found God. ‘I now know that a complete, full life for me means not only saying good-bye to Ed but also saying hello to God. I don’t think I would ever have been able to fully love myself without letting God into my life. First I let others love me, then God, and finally I was able to love myself.’
Similarly, finding my religion, Brythonic polytheism, and developing a loving relationship with my patron God, Vindos / Gwyn ap Nudd, has helped me to recover from my eating disorder and from alcohol dependency.
As I have served Him through my writing and shamanic work, Gwyn has made it increasingly clear that I need my body to be a strong vessel for inspiration from Him and my spirits. I need to be in good to health for Them and my clients. This means neither binge eating or drinking, nor restricting, nor exercising excessively. The latter is the hardest because I’ve got a hyper-active nervous system and exercise is my most effective form of stress relief. I also really enjoy it and, if I’m having a good day, I can get carried away. If I do over-exercise, I try to do my best to eat something to make up for it.
Conclusion – A Body in Service
It’s said that one of the keys to recovering from an eating disorder is shifting from how one’s body looks to what one’s body can do. I’m certainly at my happiest and have the least eating disorder thoughts when I’m immersed in something I love, whether that’s working out at the gym, writing, praying, meditating, doing shamanic work or going for a walk in my local area. This is all good so long as it’s done from a desire to serve my Gods and not to get thin, burn calories, restrict my appetites, or take my stress out on my body.
A question I keep coming back to is: ‘Who am I serving? My Gods or the ED?’
Each time I notch up a score for my Gods, I feel closer to full recovery.
For most of my life, I have struggled with an eating disorder. It began with childhood bullying when I was six years old. This resulted in binge eating and I became overweight. When I was thirteen, I began skipping meals and exercising more and lost weight, but the binging returned. Since then, my eating disorder has taken various forms, characterised by differing patterns of binge eating, restricting, over-exercising, and binge drinking. This has led to me cycling between being overweight, of a normal weight, and underweight.
Until recently, I believed I solely had binge eating disorder, and saw myself as a ‘pig’ and a ‘fat binger’. My understanding was that it had a ‘fat side’ and a ‘thin side’. So long as I was on the ‘thin side’ and in control of the binging, I was winning. I didn’t see dietary restriction and excessive exercise as a problem, even when they led to me being underweight.
It was only when I started strength training at a local gym with a personal trainer, who told me I wasn’t eating anywhere near enough to fuel my exercise, that I received an inkling that restricting my caloric intake whilst exercising a lot was an issue. It’s taken a few years to build a healthy diet and exercise routine, which has benefited me physically and mentally. In spite of this, I still have issues with fear of weight gain and feel large at a healthy weight.
A few months ago, whilst researching eating disorders for a novel, I found out that one of the characteristics of binge eating disorder is that it is not accompanied by dietary restriction. It does not have a ‘thin side’. I then saw the diagnostic criteria for anorexia – restriction of energy intake relative to requirements leading to significantly low body weight, intense fear of weight gain, and disturbance of body image. It had been my understanding that only people who were severely underweight were classed as anorexic, but this is not the case. In DSM-4 there was a weight criterion (below 17.5 BMI, which I reached a couple of times), then, in DSM-5 this was removed and anybody above 17 BMI could be classed as having mild anorexia. Could this be the name for the ‘thin side’, the secret serpent, who had hidden herself away, causing damage to my mind and body?
I decided to reach out for a clinical diagnosis from a consultant psychiatrist at a local eating disorder clinic. She told me that I did have binge eating disorder as a child and teenager, but that ended when I stopped binging on food when I turned twenty. To my surprise, she told me, primarily, I have been suffering from restricting type anorexia (there is a binging type too but this applies only to food binges and is followed by purging). Binge drinking is seen as co-occurring and is not classed as a food binge. The anorexia began when I was thirteen and applies not only to the phases when I was underweight but of a normal weight and overweight too. It is a mental illness and as such is defined by the psychological symptoms. To my shock, she told me that I still have it because I’m still calorie counting and have to ensure that I’ve burnt every calorie that I’ve eaten before I go to bed. Also, because I see myself as large at a normal weight and am terrified of weight gain.
My ‘victory’ over binge eating and binge drinking (I began giving up alcohol six years ago, have had a few lapses, but am now certain I’ve given it up for good) have come at the cost of being in the hold of the secret serpent.
The recommended treatment is eating disorder CBT (CBT-E) and I’m currently in the process of attempting to access it through the NHS. I’ve had CBT before, for anxiety, and have found it to be very practical and useful. However, whilst it’s helped managed to symptoms, it hasn’t treated the cause.
I have also been exploring these insights with my shamanic mentor and writing poetry. What follows is the story of the evolution of my eating disorder as characterised by the warring impulses of the binger and the restrictions of the secret serpent. I’m sharing it as a way of processing my diagnosis and raising awareness that anorexia can occur across the full weight range. I hope bringing the serpent from hiding will help with the healing.
Age 6 – 13 – The Comfort Eating Child
The eating disorder began when I was bullied at primary school. I wasn’t fat at first, just a little tubby, with round and rosy cheeks. But this, compounded with my social inadequacy and having a southern accent at a school on a northern council estate, led to me being singled out.
I was ashamed of being bullied and wouldn’t talk to my parents about it. They didn’t know how to comfort me. Instead, they gave me chocolate. I soon learnt to stuff down my feelings by over-eating, but this had consequences in terms of the weight gain, which led to further bullying.
Even worse were the psychological effects. The cravings. Wanting chocolate so badly when, on some basic level, I knew it was doing me harm. The desire and dread when there had been a food shop or I’d gone to choose chocolate and knew that it was in the house. The horrendous feeling of losing control and not being able to stop until I’d eaten every last thing in a packet, a selection pack, or a box. Then, the guilt, the repulsion, the feeling of the fat growing all over me. The shame. The failure. The knowledge I was going to be bullied even more badly. I kept saying this would be the last binge, but it never was.
At this point, my mum suspected that I might be autistic, but my teachers denied it because there was nothing wrong with me academically. Having been late-diagnosed with autism, I wonder if I’d have developed an eating disorder if I’d been home schooled or sent to a school for autistic people.
Age 13 – The Turnaround
The bullying continued at high school. The level of disgust at myself for being overweight became so great that something within me snapped. I decided to put my foot down. No more binging. I decided to lose weight.
I started skipping lunch and eating only half of my tea. As well as under-eating, I began cycling to the stables and worked as hard as I could at evenings and weekends. Bring on the mucking out, the sweeping, let me at that midden! I took on all the hardest jobs to burn those calories.
The weight fell off. My school skirt was soon hanging off and I had to pin it up with a safety pin. I managed to get into smaller waist jodphurs. I felt great at first, but then started suffering dizzy spells, having to retire from mucking out to sit down in the toilet or on a banking in one of the stables.
I vaguely recall people at the stables saying I looked trimmer and my parents not noticing. The fat insults stopped, but the bullying didn’t.
Age 13 – 16 – The Return of the Binger
My initial efforts at losing weight by restricting and over-exercising were confounded when the binge eating impulse returned. Since I was little, my mum and I had baked chocolate chip cookies together and this was one of my favourite binge foods. I began devouring whole trays of them.
I can’t say what the trigger was, perhaps the approach of winter nights when I couldn’t cycle to the stables anymore, perhaps simple hunger. I recall only the intensity of the shame, the guilt, which led me to stop going to the stables every evening, instead staying in to binge and read or play computer games. My self-hatred became so intense I started self-harming.
At this point in my life, the binger won. I continued skipping some lunches and eating less at tea time but this was, by far, outweighed by binging and over-eating. I went back to scoffing three-packs of Cadbury’s Caramels. At weekends, at the stables, I had a Mars Bar dipped in a cup of tea at my morning break, after lunch (a Pot Noodle) and on my afternoon break. I went to McDonalds some evenings with a friend, who also had weight issues, and we ate three Big Macs in a row followed by a large milkshake.
By the time I was sixteen years old, I was at the higher end of overweight. I found this out when said friend and I went for a riding lesson on a holiday and were both weighed and assigned to the largest and cobbiest horses.
Age 16 – 21 – The War of Two Impulses
At college, I met a new group of friends who were into alternative music. An undiagnosed autistic, chameleon-like, I decided ‘new friends, new me’. My creation of a new ‘mosher’ image combined with losing weight again, kick-started by getting my tongue pierced and not eating for three days.
I went back to skipping meals and began eating only calorie-restricted meals. I’d usually eat cereal for breakfast (to my shame I was always ravenous in the morning). If I had lunch it was diced cheese and salad, sometimes with a piece of bread. A sandwich was a binge. If I ate tea it was a piece of fish or meat with unlimited vegetables or a plate of veg with soup poured over it. The veg satisfied my binge impulse but did no favours for my bowels.
I lost three stone in around six months but, again, the binging returned. I’d be good at the beginning of the week, but as my will power failed towards the end, I’d pack away a full tub of Häagen-Dazs with a cookie in it or three Pot Noodles in a row. The binging was always worst after alcohol, when I’d lose control and eat all the leftovers at a buffet or a huge kebab. When I’d been out and stayed over at some else’s house, in the morning, the first question that I would ask, in panic, was “What did I eat?” The day after drinking, I ate not only one but two plates of beans and cheese on toast for lunch. Binges were often followed by episodes of self-harm.
By this time I had already started drinking at weekends and smoking cigarettes and weed. I began drinking more regularly, usually vodka, to help me socialise, to regulate my anxiety and to help me sleep. I also discovered other drugs such as LSD, ecstasy and amphetamine. The use of the latter and going out dancing all night led to further weight loss.
After not being able to cope living away at university in Liverpool due to my autism combined with the unhealthy habits of under-eating then drinking heavily and binge eating, I returned home and went to UCLan.
Finally, I got the food binging under control, reducing my binges from walking from shop to shop buying chocolate bars, to diet snack bars, to diet drinks and sugar-free sweets. The latter two continued as binge substitutes.
Age 21 – 24 – Floating Away
My mental health hit an all-time low when I was in the second year of university. I was taking a lot of drugs, drinking heavily, and not eating enough. I struggled with dizziness, feeling faint, and panic attacks. I was barely in my body and felt like I was floating away. I suffered from derealisation and thought I was going mad. I couldn’t sleep. I had no idea what was real and what was not. I feared I was trapped in a nightmare world of my own imagining. I had black-outs and am still missing memories.
When I reached out to a psychiatrist I was turned away, even though I was struggling with self-harm and suicidal ideation, as I hadn’t attempted suicide.
Luckily, I wasn’t tempted to attempt suicide in order to get help. I found a more understanding GP, who prescribed beta blockers for the panic attacks and sleeping tablets. When the beta blockers didn’t work, just making me colder and number, and the sleeping tablets exacerbated my panic as they gave me the feeling of sinking down into sleep during the day, she put me on an anti-depressant recommended for treating anxiety called Venlafaxine.
I didn’t mention that I was under-eating as I saw myself as a fat pig. It wasn’t picked up on that I was slightly underweight. In fact, the GP prescribed exercise! The Venlafaxine helped and I left university with a first class degree.
Whilst finishing my degree and pursuing my MA, I exercised moderately. I joined a gym and did a bit of cardio and aerobics and took up taekwondo. I discovered it allowed me to eat a little more and stay at a low weight.
Age 25 – 26 – Mad for Exercise
When I failed to gain funding for a PhD, I was gutted. Forced to take a year out to re-apply for self-funded studies, I started over-exercising. I ran or did cardio in the morning, then worked a cleaning job in the afternoon. At weekends, I went on long bike rides. I didn’t know the meaning of a rest day. The exercise, the decreasing numbers on the scales and feeling lighter eased the pain of failure.
For the first time, I was noticeably underweight and people started commenting. When I went out running, I heard one of a group of lads say “Look at the size of her arse,” and thought he meant it was big until another of them added, “ugh, look how skinny she is.” My friend’s boyfriend’s mum, who went to the same gym, voiced her concerns about how I went at it on the cross-trainer. My mum was also concerned. I didn’t see it.
My periods stopped. I was tested for polycystic ovaries, which I didn’t have. That I was underweight wasn’t seen as a concern, perhaps because I was a runner.
Fortunately, although it didn’t feel it at the time, my over-exercising was put an end to by pattelofemoral syndrome (runner’s knee). No amount of icing, taping or acupuncture would cure it. I was forced to slow down.
Age 27 – 30 – Horses and Cider
I began a self-funded PhD and returned to Oakfield to work as a riding instructor to fund it but couldn’t cope with working and studying full time. Thus, I ditched academia in favour of working with horses full time. I loved the work and the horses and the exercise helped me to maintain a lowish weight.
Whilst I was at Oakfield, I managed to limit my drinking to a bottle of wine mid-week and a couple at the weekend. However, when I moved to Hertfordshire to work as an event groom, the head girl, who I lived with in a mobile home, was not only a fellow drunkard but a cider drinker. I got a taste for cider, drank far too much, and began to gain weight again. This continued when I moved back home and took a job as head girl at a dressage stud.
This job proved to be too high pressure. Thus, I abandoned my equine career in favour of attempting to fulfil my long-time ambition of becoming an author.
Age 30 – 34 – The Drunken Bard
I worked a variety of physical jobs including shelf-stacking at a supermarket, packing at Oakfield Saddlery and cleaning to support myself as I wrote a novel and began writing and performing poetry. This did not prove to be enough to work off the amount of calories I was consuming from alcohol.
At this point, I found my spiritual path as a bard, then as an awenydd, in the Brythonic tradition. For the first time since my teens, the binger over-ruled the infuriated hissing of the serpent. I was a Brythonic bard. A warrior woman. A bit of black eye-liner. A drink before I went out. I didn’t care if I was fat.
I loosened up on dieting. I joined a local Pagan Society and attended pie nights and started drinking beer. A friend introduced me to craft beer – chocolate stout, coffee porters, triple-hopped IPAs, Belgian beers such as Trippels, Dubbels and Quadrupels. Kwak, Maredsous, Leffe Brunne and Blonde. Some of those beers contained more than 400 calories! I drank heavily up to five times a week and sometimes from noon on a Saturday until the early hours of the next morning and this all led to me being borderline overweight.
The serpent seethed. I drowned her out. Yet, in moments of sobriety, I was unhappy with my size. Feeling down and desperate, I decided to try running again.
Age 35 – 39 Running Thin
With better shoes, at the beginning, my knee held out. And I genuinely enjoyed running. The sense of freedom. The runner’s high. It suited my power animal – Horse. It brought me closer to the Gods and spirits.
I got up to running 30 miles a week and to half marathons. As intended, I lost a couple of stone and got down to a lowish normal weight. However, under-fuelling food-wise for the amount I was running combined with heavy drinking took its toll on my body. I struggled with IBS and ended up with a stress fracture in my right foot. That put an end to running for a good while.
Age 39 – 40 – The Rake
When I realised that, in spite of my efforts with writing and performing poetry and succeeding in publishing three books, I was never going to make a living from my writing, I attempted to pursue a career in conservation. This fit with my spiritual path and the volunteering I had been doing in my local area. (And, yes, you guessed it, outdoor work felt like a good method of staying slim).
At the age of 39, realising that drinking was having an impact on my plans to volunteer my way into conservation, I gave it up for the first time. With the calories from alcohol gone, the weight fell off. I lost six pounds in a month. I lost another six pounds in a couple of months. My periods stopped again.
This was at the time Covid hit. With no volunteering and no job, I had little to do but exercise. I gutted the house. I worked in the garden. In spite of the lockdown rules, I went for long walks around my locality.
When I went back to volunteering at Brockholes, I was underweight and without the extra calories from alcohol was eating nowhere enough to sustain cycling there and back and doing outdoor work. I was told I looked like a rake when I was standing next to a rake. I came near to fainting and falling off my bike on the way home. I suffered from the cold. I developed Raynaud’s.
When I started a paid traineeship on the Manchester Mosslands, I started drinking again due to the stress and, to burn the calories, went back to running. As winter was approaching and I was struggling with runner’s knee and deep gluteal syndrome, I decided to join a local gym and try strength training.
Age 40 – 44 Strength
When I started at the gym and signed up with my PT, I was certain she would say I needed to lose weight. I’d put on over half a stone by drinking beer again. Thus, I was surprised when she told me I was eating nowhere near enough calories to cover running or going to the gym early in the morning then doing outdoor work. I could barely believe her. She went through how and where to add in extra calories, mainly in protein, which would help me feel fuller for longer and help me build muscle to support my joints.
As she had promised, I didn’t gain too much weight, just a few pounds in muscle. I felt a lot better and stronger physically and mentally. I stopped feeling fatigued and light-headed and haven’t had a panic attack since. I also managed to cut down on drinking as I preferred feeling good for my workouts.
However, I became incredibly attached to my eating and gym routine. This impacted the ecology job which I took when I finished my traineeship. Running or doing strength training early in the morning did not fit well with doing great crested newt surveys at night. I soon realised that, in any case, night work did not suit me as an autistic person who needs a regular sleep pattern and is naturally an early riser. Because of this, I left the job.
Age 41 – 44 – Monasticism and Shamanic Training
Retreating, I experimented with living as a nun and saw my food and exercise regime as a form of asceticism that fit with my monastic ideals. I practiced other forms of restriction such as paring down my wardrobe, getting rid of most of my books and cutting out most forms of entertainment. The secret serpent, unable to restrict my food intake, liked this very much.
I also began training as a shamanic practitioner. Initially, this took place in Devon with an organisation I have now left called the Sacred Trust. I was notably the only one who got up early to walk for six miles and took my own weights so I could get some of my strength training exercises in.
More positively, as I deepened into monasticism and worked with my mentor, Jayne Johnson, a shamanic practitioner and embodied relational therapist who took me on as a shamanic apprentice when I left the Sacred Trust for ethical reasons, I developed a number of practices that helped me develop a better relationship with my body. These included meditation, breathwork, mindfulness, and nervous system regulation based on polyvagal theory.
These stood me in good stead when my research revealed the true nature of my eating disorder and I had to revisit the past in order to piece together the story. This was incredibly painful as I’d forgotten a lot of the binges. I had to ask my mum what I ate as a child and was appalled as the memories returned, in conscious recollections, in unconscious moments, in dreams. Coming to acknowledge what a great impact under-eating and its effects had on my education and career came as a shock and formed a wake-up call.
Age 44 – Diagnosis and Lash Back
I was initially uncertain about whether to reach out for a diagnosis. Whilst the diagnostic criteria suggested I might have mild anorexia, the serpent voice in my head hissed its denial. “Nonsense.” “You’re too large.” “You’re too old.”
Since my diagnosis has been confirmed and the identity of the voice has been outed, in contrast to my expectations, it has initially got louder. “You’re a crap anorexic.” “You’re the fattest and oldest anorexic in the world.” “Look at how humungous you’ve got by doing all that strength training.” “You’re big and brawny.” “Look at your huge red face.” “You still look like a fat drunk.”
It remains a constant battle not to give in to the urge to over-exercise when I’m stressed and, if I do give in, to eat something to make up for it.
Towards Recovery
Recovery from an eating disorder looks different for every person. Some people recover completely. Others settle for learning to manage their eating disorder. I know full well that, because I’m autistic and my food and exercise habits are so bound up with the restrictive and repetitive behaviours that form the foundation of my life, I’m unlikely to be able to follow others in embracing intuitive eating and exercising and being ‘free’ from regulated patterns. What looks like freedom to some people scares the shit out of me! Instead, I have a greater hope of building on the work I’ve done already to enlist my autism in building healthy habits and ditching less healthy ones.
Many books and websites recommend separating from an eating disorder and learning to argue with it and stand up to it. I agree with this to a certain degree. It’s very easy to become identified with an eating disorder – to see oneself as a binger or as an anorexic and to be over-powered by these parts. Seeing these are just parts of oneself and not the whole is very important.
However, pathologising the eating disorder as entirely separate, like a disease, or a domineering partner or boss, and simply attempting to get rid of it does not strike me as a good strategy. In my experience, parts that are cut off just come back in different guises to bite you.
The way forward I have been taking with my shamanic mentor has been getting to know the binging and restricting parts and the function they have played. It’s my understanding that my binge eating began as a response to the trauma of bullying because I was not taught better coping mechanisms. Unfortunately, that caused more trauma in the form of my eating getting out of control. I still have nightmares about eating binge foods. The restricting part then came in to help me control the binger but herself got out of control, with under-eating leading to more trauma in the form of light-headedness, feeling faint, panic attack, black-outs and the stress of over-exercising on my body.
Thus, central to recovery is learning better coping mechanisms for dealing with trauma and the stress and overwhelm of living as an autistic person in a busy social world. Meditation and mindfulness have worked to bring me into the present moment rather than ruminating on failures of the past or feeling anxious about failing in the future. Breathwork, particularly breath retentions, has helped slow and still my mind. Slowing down and being in my body, particularly when exercising, have made me less prone to pushing too hard.
I’ve found that researching physiology, anatomy and nutrition and gaining an understanding of my body and how wonderful and intelligent it and its inner processes are have made me less likely to mistreat it. This, combined with shamanic journeys into my body have helped me to relate to it much better.
Having an animistic approach to food and an understanding of the complex web of life in which it and eating are enmeshed has instilled greater gratitude.
I have also done shamanic work dialoguing with, meditating on and journeying to the binger and the secret serpent. The former has appeared as a pup, a hungry hound and a ravening monster and I see him as representing my appetite. The latter appears as a woman in black or as a black serpent. Sometimes she is wound around me like a snake or a Siamese twin who is inseparable. I see her as representing restriction of appetite. Both are necessary and serve a function but can be deadly when they seize control. I’m hoping that building relationships with them will help me keep them in balance.
Another facet is that an eating disorder is a time thief. Obsessing about food and exercise takes time away from my relationship with my Gods and spirits. Thus, for me, recovery is about winning back more time for devotion and shamanic practice. In this, I can call for help from my patron God and spirit helpers.
I see the eating disorder as both a curse and a gift – it’s done a lot of damage but it’s also taught me a lot about the binging and restricting impulses that exist within me, within each one of us, and within our society and culture at large. So far I’ve done a lot of good work and I have a lot more work to do.
I’d be interested to hear about how others have dealt with eating disorders and about your relationship with food and exercise from a spiritual perspective.